Cognitive health
The relationship between
mental health and cognitive health
Dr. Kieran Rea
Scientific Director at Atlantia Clinical Trials, Cork, Ireland
About the Author
Dr. Kieran Rea
Dr. Kieran Rea is the Scientific Director at Atlantia Clinical Trials, with expertise in neuropharmacology, microbiome research, and clinical trial design. Holding a PhD in Neuropharmacology, he has led research on cannabinoids, cognition, and pain. Before joining Atlantia, he held leadership roles at Eli Lilly, Deerland Probiotics & Enzymes, and ADM, overseeing clinical trials and R&D.

KEYWORDS
Cognitive health
Mental health
Neurodevelopment
Gut-brain axis
Cognitive assessment
Dietary supplements
Abstract
Designing clinical trials for mental health, particularly cognitive health, involves navigating unique challenges and opportunities that can significantly impact trial outcomes. Dr. Kieran Rea will explore key considerations, including the complexities of recruiting diverse populations, addressing stigma surrounding mental health, and ensuring ethical approaches to informed consent. The talk will also highlight opportunities to leverage digital tools for remote monitoring, personalize interventions for specific mental health conditions, and improve participant retention through patient-centered strategies. Combining literature review and consensus withemerging trends, Dr. Rea will provide actionable insights for creating effective, compassionate trial designs that advance mental health care.
Introduction
Mental health refers to our emotional, psychological, social well-being and cognitive function. It encompasses our thoughts, feelings, and behaviours, how we act and react, and how we perceive and interact with the world. There are a number of mental health disorders that can range from mild to severe including anxiety disorders (e.g. general anxiety disorder, panic disorders, phobias), mood disorders (e.g. depression, bipolar disorder), obsessive-compulsive disorder and related disorders, post-traumatic stress disorder, psychotic disorders (e.g. schizophrenia), eating disorders (e.g. anorexia nervosa, bulimia) and neurodevelopmental (e.g. autism spectrum disorder, ADHD) and neurodegenerative disorders (e.g. Parkinson’s disease and Alzheimer’s) (1).
Our mental health impacts our ability to cope with stress, handle challenges, and maintain healthy relationships. Emotional wellbeing entails our perception and appropriate management of emotions in response to life experiences. Psychological wellbeing includes our cognitive health, self-esteem, resilience and overall satisfaction with life; while social wellbeing refers to our relationships and social interactions and sense of belonging. Mental and cognitive health are intertwined, where poor emotional health can hinder cognitive function, and cognitive issues can impact emotional well-being.
Cognition is an overarching term covering many complex and interactive mental processes that occur in the brain, and refers to the status of our brain’s functionality and the processes that enable us to acquire, process, store, retrieve and appropriately utilise information (2, 3). Cognitive impairment can affect memory, attention, problem-solving, processing speed, visual-spatial skills, executive function, sensory perception, communication, decision-making, and learning abilities, impacting daily life and mental well-being. In this review we will discuss some actionable insights for designing more effective clinical studies to address mental health care and cognitive performance using prior learnings and advances in assessment tools.

Cognition across the lifespan
Cognition changes throughout the lifespan from birth to old age, and several factors influence how our cognitive abilities evolve over time. These factors can vary widely and include both biological and environmental elements. For example, genetics play a significant role in shaping our cognitive abilities with inherited traits influencing intelligence, memory, brain development, and susceptibility to cognitive decline or disorders associated with cognitive health. In early life, the brain undergoes rapid development, with the cells in our brains (neurons) forming synaptic connections and undergoing pruning and maturation. From infancy, cognitive abilities like communication and motor skills emerge affecting learning, memory, attention, and problem-solving abilities, while in later life many synaptic connections are lost and the efficiency of synaptic neurotransmission can deteriorate, and cognitive decline can occur (4-6). Dietary nutrients and supplements, particularly microbiome modulators (prebiotics, probiotics, postbiotics), those rich in omega-3 fatty acids (e.g. DHA, EPA), antioxidants (e.g. carotenoids, phenolic acids, flavonoids), phospholipids (7) (e.g. phosphatidylcholine, phosphatidyl serine, phosphatidyl ethanolamine, phosphatidyl inositol and sphingomyelin) and several vitamins (e.g. A, B6, B9, B12, C, D3 and E) and minerals (e.g. iodine, iron, magnesium) amongst others have been shown to support the development, maturation and maintenance of cognitive health throughout the lifespan from early life to ageing including memory, attention, processing speed, visual-spatial skills, executive function, sensory perception, stress management, language and social cognition (5, 8). Alongside dietary nutrition, environmental factors including education, social relationships, early-life experiences, hormonal changes, exercise, sleep, mental health status, lifelong learning and mental stimulation (reading, puzzles, music) are all critical contributors to cognitive health in the development, maturation and maintenance of healthy cognitive function.
Microbiome-Gut-Brain communication
The microbiota-gut-brain connection is an emerging area of research that explores how the gut microbiota (the community of microorganisms living in the digestive system) can influence brain function, cognition, mood, and behaviour. Factors that impact this first early seeding of our gut microbes are whether we are vaginally delivered getting vertical transmission of vaginal microbes from our mothers or whether we undergo caesarean section getting exposure to skin microbes in the first instance. Shortly after delivery, another important contributing factor to gut microbiota development is whether we are breastfed or bottle fed, as there are many nutrients present (including distinct human milk oligosaccharides) in our mother’s milk that may be absent in bottle feeding that act like prebiotics nourishing different families of microbes. Next comes the weaning period, where we first start getting exposure to solid foods, and the reduction of breastmilk or bottle-milk, and thereafter the exposure to different food-types profoundly impacts our gut microbe development. Furthermore, medication in early life, particularly antibiotics can impact early gut microbiota development. As such, the microbiota of each individual is unique, like a fingerprint that has developed as we get exposed to microbes in our environment (5).
Along our gastrointestinal tract we have millions of microbes that communicate with the lining of the gut and can influence the bi-directional communication between the gut and brain (5). Interestingly, there are many aspects of our diet that we humans as a host cannot metabolise, and are reliant on the microbes that reside in our gut to breakdown by enzymatic means (e.g. digestion-resistant fibres that get metabolised in the large intestine into molecules such as short chain fatty acids, and branched chain fatty acids) (9) that we as hosts can then utilise in metabolism. Similarly, gut microbes can impact the pharmacodynamics and pharmacokinetics of pharmacological agents; and vice versa, the gut microbes can be altered by various drug types (e.g. antibiotics, antidepressants, antipsychotics amongst others), and this fascinating area of research (pharmacomicrobiomics) is currently gaining much more interest.
Several studies (both preclinical and clinical) have looked into the microbiome to determine if any imbalances are associated with disease-related states or cognitive health, but there is no clear correlation for any keystone gut bacteria or microbiome modulator for improved cognitive health. Psychobiotics is a term used for probiotics that have been developed for effects on mental health, and there is some evidence for some probiotics in cognitive health mostly lactobacilli, bifidobacteria and bacteriodes species but further evidence is required to clearly demonstrate an improvement in cognitive health (5, 10). Some interesting preclinical studies comparing naïve control animals to germ-free or antibiotic treated animals have demonstrated that our gut microbes contribute to myelin thickness of neurons, spine density of neurons, alterations in gene transcription in the amygdala, hypertrophy of neurons, and in the maturity, function and maintenance of microglia in the brain (5, 11).
Biomarkers to assess cognitive health
Identifying biomarkers for cognitive health is crucial for diagnosing and tracking cognitive decline. Biomarkers like amyloid plaques, tau protein, neurofibrillary tangles and neurofilament light chains have been linked to neurodegenerative diseases like Alzheimer's. These markers are detectable in cerebrospinal fluid (CSF) or brain scans, but their role in cognitive impairment is still unclear. Biomarkers like BDNF, synaptic proteins, cytokines, microglia, myelin and other markers of neuronal health also show promise in diagnosing cognitive disorders, but further research is required to establish causality and improve diagnostic accuracy (12, 13, 14).
Pharmaceuticals in cognitive health
Pharmaceuticals aimed at improving cognition have been studied for conditions like Alzheimer's and Parkinson's disease. Cholinesterase inhibitors (e.g., Donepezil, Rivastigmine, Galantamine) and NMDA receptor antagonists (e.g., Memantine) have shown some efficacy in slowing cognitive decline, though their mechanisms are not fully understood (15). Psychostimulants like amphetamines (Adderall), methylphenidate and modafinil have been used to improve alertness, attention and executive function in certain contexts (3).
Clinical practices in cognitive assessment
Assessing cognitive health involves baseline testing to track changes over time. A multidisciplinary approach, including neurologists, psychologists, and therapists, is often used. Various neuropsychological tools, such as the Mini-Mental State Examination (MMSE) and Montreal Cognitive Assessment (MoCA), are commonly used to measure cognition. Computerized tests like CANTAB and Cogstate provide objective assessments of memory, attention, and executive function. Neuroimaging methods like MRI, CT scans, and PET scans can visualize structural and functional changes in the brain (16, 17).
Electrophysiological methods like EEG and MEG provide real-time insights into brain activity, useful in studying memory and attention. EEG is particularly useful in detecting abnormal brain wave patterns in conditions like ADHD, while MEG measures neuronal activity in higher cognitive functions.
With the rise of digital tools, several apps have been designed to boost and track brain function including memory, language skills, executive function, processing speed, attention, puzzles and problem solving, as well as mindfulness apps for stress management, and techniques to improve sleep, focus and overall mental wellbeing. Virtual reality headsets are also being used to improve cognitive abilities including higher executive functioning, hand-eye coordination and spatial navigation.
Designing a clinical study to assess cognitive health
There are several factors to consider when designing a clinical study for cognitive assessment (Figure 1).
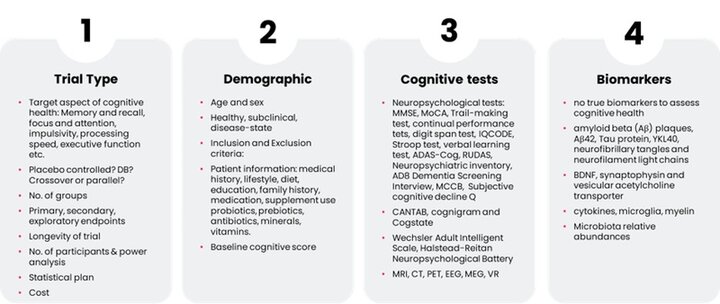
Figure 1. Considerations for clinical study design targeting cognitive assessment
In the first instance, the sponsors must decide whether the study in a ‘healthy’ population, a ‘mild to moderate/subclinical’ population, or a disease state; and at what stage of disease (e.g. early onset versus full-blown dementia). Depending on the objectives, it should be decided whether the study is a parallel or crossover study design, is there a control group(s), and whether the study is blinded. Careful consideration must be given to the criteria for inclusion and exclusion, and this should be done with clear understanding of what criteria are accepted by different regulatory bodies in different territories. Another key consideration is what aspect of cognition the trial should be focussed on. Important co-factors include gender (for some disorders, there is a bias towards gender), age and age range, educational background, role of the caregiver (if in a disease population) and baseline cognitive scoring at this point. Cognition encompasses memory, attention, processing speed, visual-spatial skills, executive function, sensory perception, language and social cognition amongst others, so the sponsor should clearly identify what is the primary endpoint for assessment based off what is known about the treatment or intervention from preclinical assessments and/or information in the literature. For example, should the study objective be to assess a specific cognitive domain (e.g., memory, executive function perhaps by using CANTAB or questionnaire or battery-based approach) or a global cognitive score (e.g., MMSE, ADAS-Cog). The sponsor should also determine the duration of the study, what secondary or exploratory endpoints are they going to target, and whether methodologies such as wearable devices, apps, MRI, PET, CT scans, EEGs, MEGs, questionnaires, skillset batteries will be employed, as well as deciding whether any biomarkers are going to be assessed and from what sample types (e.g. blood, stool, urine, biopsies). To improve participant retention one could consider the number of timepoints and whether the study can be conducted remotely, with prompts from the study co-ordinator, and potentially the support of apps to monitor and track trial progress. Once the target demographic,study duration and primary, secondary or exploratory endpoints have been identified, a power analysis should be conducted with expected inter-individual variability also considered to determine the number of participants to be included in the study. Thereafter a statistical analysis plan should be identified, after which ethics approval needs to be sought, and the trial should be registered on a relevant database (e.g. clinicaltrials.gov) prior to commencement of the study. The study should also be registered with a database such as Cochrane Dementia and Cognitive Improvement Group’s (CDCIG’s) register of all dementia trials, ALOIS. ALOIS is a freely accessible electronic database whose aim is to collate information on all trials with a dementia or cognition focus.
Conclusion
Cognitive health is critical across the lifespan, with factors like genetics and life experiences shaping cognitive abilities. While some factors are uncontrollable, dietary interventions, exercise, sleep management, and stress reduction can support healthy cognitive aging.
From a consumer perspective the main areas of interest for dietary supplements in cognition include memory, attention, stress management, mood, energy and mental wellbeing. The microbiome-gut-brain axis plays an emerging role in brain function, with research into probiotics and diet suggesting potential benefits. However, more work is needed to understand the full impact of gut health on cognitive outcomes.
In this article we introduce the biomarkers, digital tools, and intervention strategies will continue to advance the field of cognitive health. A multi-targeted approach that incorporates diet (and supplements) with exercise, sleep, and stress management offers the most promising strategy for maintaining cognitive health throughout the lifespan.
References and notes
References and notes
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). https://doi.org/10.1176/appi.books.9780890425596
- Eysenck MW. Applied cognitive psychology: Implications of cognitive psychology for clinical psychology and psychotherapy. J Clin Psychol. 2004;60(4):393-404.
- Bostrom N, Sandberg A. Cognitive enhancement: methods, ethics, regulatory challenges. Sci Eng Ethics. 2009;15(3):311-41.
- Garcia-Garcia I, Donica O, Cohen AA, Gonseth Nussle S, Heini A, Nussle S, et al. Maintaining brain health across the lifespan. Neurosci Biobehav Rev. 2023;153:105365.
- Cryan JF, O'Riordan KJ, Cowan CSM, Sandhu KV, Bastiaanssen TFS, Boehme M, et al. The Microbiota-Gut-Brain Axis. Physiol Rev. 2019;99(4):1877-2013.
- Dinan TG, Cryan JF. Gut instincts: microbiota as a key regulator of brain development, ageing and neurodegeneration. J Physiol. 2017;595(2):489-503.
- Schverer M, O'Mahony SM, O'Riordan KJ, Donoso F, Roy BL, Stanton C, Dinan TG, Schellekens H, Cryan JF. Dietary phospholipids: Role in cognitive processes across the lifespan. Neurosci Biobehav Rev. 2020 Apr;111:183-193.
- Fekete M, Lehoczki A, Tarantini S, Fazekas-Pongor V, Csípő T, Csizmadia Z, Varga JT. Improving Cognitive Function with Nutritional Supplements in Aging: A Comprehensive Narrative Review of Clinical Studies Investigating the Effects of Vitamins, Minerals, Antioxidants, and Other Dietary Supplements. Nutrients. 2023 Dec 15;15(24):5116.
- Moseholm KF, Meineche JT, Jensen MK. The potential of circulating nonesterified fatty acids and sphingolipids in the biological understanding of cognitive decline and dementia. Curr Opin Lipidol. 2025;36(1):27-37.
- Sarkar A, Lehto SM, Harty S, Dinan TG, Cryan JF, Burnet PWJ. Psychobiotics and the Manipulation of Bacteria-Gut-Brain Signals. Trends Neurosci. 2016;39(11):763-81.
- Nohesara S, Abdolmaleky HM, Dickerson F, Pinto-Tomas AA, Jeste DV, Thiagalingam S. Maternal Gut Microbiome-Mediated Epigenetic Modifications in Cognitive Development and Impairments: A New Frontier for Therapeutic Innovation. Nutrients. 2024;16(24).
- Shah J, Krell-Roesch J, Forzani E, Knopman DS, Jack CR, Petersen RC, et al. Predicting cognitive decline from neuropsychiatric symptoms and Alzheimer's disease biomarkers: A machine learning approach to a population-based data. J Alzheimers Dis. 2025:13872877241306654.
- Shah J, Rahman Siddiquee MM, Krell-Roesch J, Syrjanen JA, Kremers WK, Vassilaki M, et al. Neuropsychiatric Symptoms and Commonly Used Biomarkers of Alzheimer's Disease: A Literature Review from a Machine Learning Perspective. J Alzheimers Dis. 2023;92(4):1131-46.
- Hampel H, Hu Y, Cummings J, Mattke S, Iwatsubo T, Nakamura A, et al. Blood-based biomarkers for Alzheimer's disease: Current state and future use in a transformed global healthcare landscape. Neuron. 2023;111(18):2781-99.
- Di Santo SG, Prinelli F, Adorni F, Caltagirone C, Musicco M. A meta-analysis of the efficacy of donepezil, rivastigmine, galantamine, and memantine in relation to severity of Alzheimer's disease. J Alzheimers Dis. 2013;35(2):349-61.
- Noel-Storr AH, Flicker L, Ritchie CW, Nguyen GH, Gupta T, Wood P, et al. Systematic review of the body of evidence for the use of biomarkers in the diagnosis of dementia. Alzheimers Dement. 2013;9(3):e96-e105.
- Harrison JK, Noel-Storr AH, Demeyere N, Reynish EL, Quinn TJ. Outcomes measures in a decade of dementia and mild cognitive impairment trials. Alzheimers Res Ther. 2016;8(1):48.
